Anotace
Úvod. Výběr vozíku, jeho nastavení a sedací polštář zásadně
ovlivňují mobilitu člověka s lézí míšní, vznik patologie
postury i dekubitů.
Metody. 90 pacientů s lézí míšní (LM), mobilitou na mechanickém
vozíku (MIV), starších 18 let, 69 (76,7 %) mužů a 21 (23,3 %)
žen, bylo vyšetřeno ve spinální ambulanci celoživotní péče FN
Brno 2014-2017. Při sezení ve vozíku byl měřen tlak na sedacím
polštáři pomocí pressure mapping system Conformat Evolution
firmy Tekscan.
Výsledky. U 29 (32,2 %) pacientů byl zjištěn tlak ≥ 100 mmHg
současně pod oběma hrboly sedacích kostí (p<0,001). U 28 (31,1
%) pacientů byl současně pod oběma hrboly sedacích kostí
zjištěn tlak menší než 100 mmHg (p<0,001). U 37 (41,1 %)
pacientů byl zjištěn dekubitus v oblasti kompromitované sezením
(p<0,001). Celkem bylo zjištěno 69 dekubitů, z nichž 47 (68,1
%) bylo pod hrbolem sedací kosti (p<0,001). U 67 (74,4 %)
pacientů byla při sezení ve vozíku verifiková obliquita pánve
(p<0,001) a přítomnost dekubitu u 21 (23,3 %) pacientů sedících
s obliquitou (p<0,001). U pacientů sedících s obliquitou pánve
se vyskytlo 53 (76,8 %) ze všech dekubitů (p<0,001). 14 (15,5
%) pacientů sedících s obliquitou pánve mělo vyšší tlak pod
hrbolem sedací kosti na straně druhé, než byla obliquita. U u
71 (78,9 %) pacientů byla zjištěna retroflexe pánve (p<0,001).
U 50 (55,6 %) pacientů sedících s retroflexí pánve byla
patologie rozložení tlaku (p<0,001). 24 (26,7 %) pacientů
sedících s retroflexí pánve mělo dekubitus (p<0,001). Ze 71
(78,9 %) pacientů s retroflexí pánve má 63 (70 %) pacientů
rozdíl tlaku mezi stejnostranným hrbolem sedací kosti a stehnem
30mmHg a více na straně pravé i levé (p<0,001). U 71 (78,9 %)
pacientů sedících s retroflexí pánve byla u 60 (66,7%) pacientů
zjištěna kyfotizace bederní páteře a celé postury (p<0,001). Ze
32 (35,6 %) tetrapostižených mělo 8 (8,8 %) pacientů dekubity a
všichni byli s kompletní motorickou LM (AIS A , AIS B). Ze 32
(35,6 %) tetrapostižených mělo 20 (22,2 %) pacientů patologii
rozložení tlaku pod hrboly sedacích kostí (p<0,001). Z 58 (64,4
%) parapostižených pacientů mělo 44 (48,9 %) pacientů patologii
rozložení tlaku pod hrboly sedacích kostí (p<0,001) a u 22
(24,4 %) pacientů (p<0,001) se vyskytlo celkem 40 (58 %)
dekubitů (p<0,001), z nichž 32 (46,4 %) bylo pod hrboly
sedacích kostí (p<0,001).
Závěr. Nehomogenní rozložení tlaku na sedacím polštáři a tlak ≥
100 mmHg je výrazným rizikovým prvkem pro vznik dekubitů a
patologii postury. Dekubity vznikají nejčastěji v oblasti
hrbolů sedacích kostí. …víceméně
Abstract
Background. The choice and adjustment of wheelchair and seating
cushion affects essentially
spinal cord injury (SCI) persons' mobility, formation of their
postural pathology and pressure ulcers.
Methods. A set of 90 patients with SCI, mobility in manual
wheelchair, older 18 years, 69 (76,7 %) men and 21 (23,3 %)
women, were examined at SCI outpatient centre of University
Hospital Brno 2014-2017. The pressure on seating cushion was
analysed during seating in wheelchair using pressure mapping
system Conformat Evolution, Tekscan, Inc.
Results. The pressure 100 mmHg and higher under both ischal
tuberosities at the same time was found in 29 (32,2 %) patients
(p<0,001). The pressure lower than 100 mmHg under both ischal
tuberosities at the same time was found in 28 (31,1 %) patients
(p<0,001). A pressure sore at area compromised by seating was
verified in 37 (41,1 %) patients (p<0,001). A total of 69
pressure ulcers were detected, of which 47 (68,1 %) was under
ischial tuberosity (p<0,001). A pelvic obliquity was analysed
in 67 (74,4 %) patients seated in a wheelchair (p<0,001) and 21
(23,3 %) patients seated with obliquity had a pressure ulcer
(p<0,001). 53 (76,8 %) of pressure ulcers were found in
patients seated with pelvic obliquity (p<0,001). 14 (15,5 %)
patients seated with pelvic obliquity had a higher pressure
under opposite ischial tuberosity then the obliquity was. In 71
(78,9 %) patients was analysed posterior pelvic tilt (p<0,001).
In 50 (55,6 %) patients seated with posterior pelvic tilt was a
pathology of the distribution of pressure on seat cushion
(p<0,001). 24 (26,7 %) patients seated with posterior pelvic
tilt had a pressure ulcer (p<0,001). A pressure difference
under equilateral thigh and ischial tuberosity greater than 30
mmHg on the right and left side was found in 63 (70 %) patients
from 71 (78,9 %) patients seated with posterior pelvic tilt
(p<0,001). A kyphotic lumbal vertebral column and whole
kyphotic posture was found in 60 (66,7 %) patients from 71
(78,9 %) seated with posterior pelvic tilt (p<0,001). 32 (35,6
%) patients were tetraplegics, 8 (8,8 %) of them had pressure
ulcer and complete motor lesion AIS A or AIS B. A pathological
pressure distribution under ischial tuberositis (p<0,001) was
analysed in 20 (22,2 %) patients from 32 (35,6 %) tetraplegics.
A pathological pressure distribution under ischial tuberositis
(p<0,001) was analysed in 44 (48,9 %) patients from 58 (64,4 %)
paraplegics and 22 (24,4 %) patients (p<0,001) had 40 (58 %)
pressure ulcers (p<0,001), from which 32 (46,4 %) were under
ischial tuberosities (p<0,001).
Conclusions. Non-homogeneous pressure distribution and the
pressure 100 mmHg and higher
on seating cushion is very strong risk factor of pressure
ulcers and postural pathology. Pressure ulcers are most
frequently located under ischal tuberosities. …víceméně
 čeština
čeština
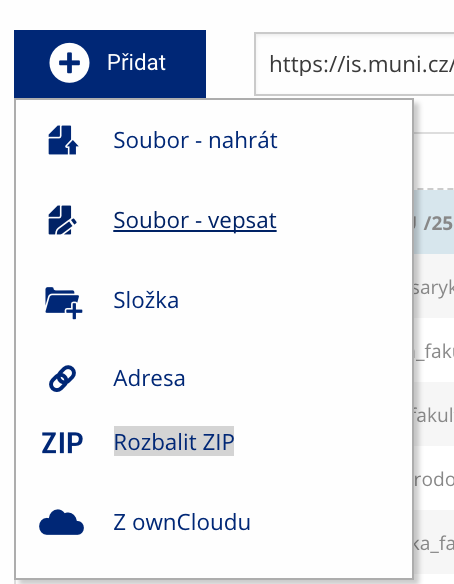 Soubor nebo složku lze nahrát pomocí tlačítka Přidat.
Soubor nebo složku lze nahrát pomocí tlačítka Přidat.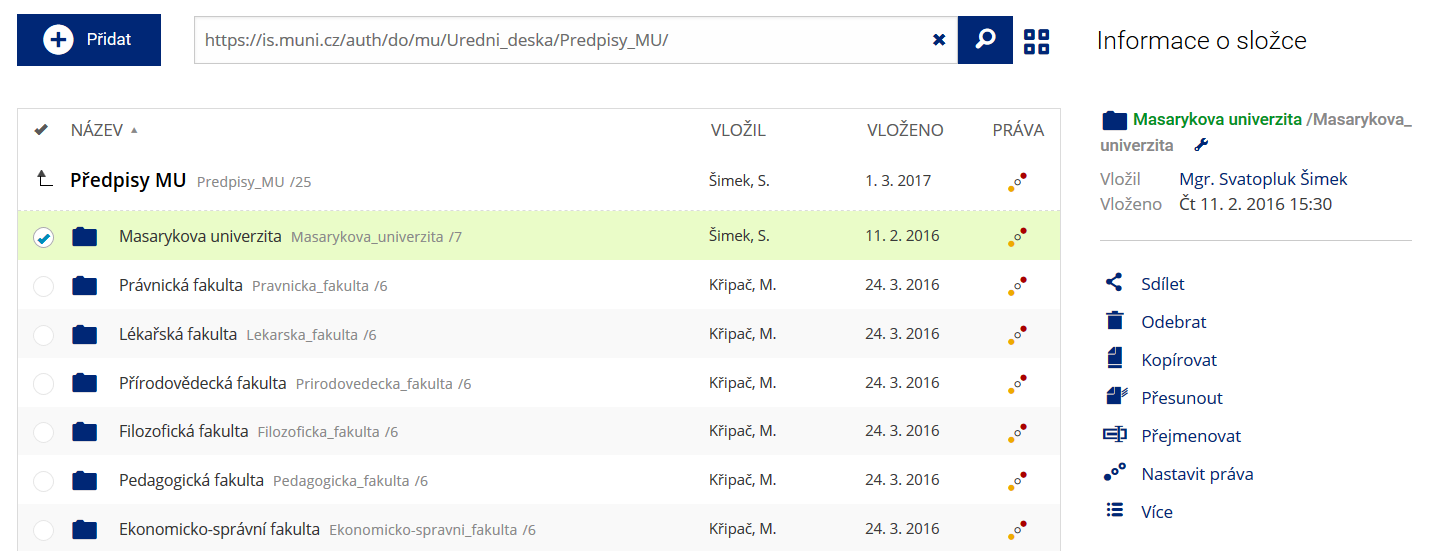 Podrobnosti lze zjistit označením příslušného řádku.
Podrobnosti lze zjistit označením příslušného řádku.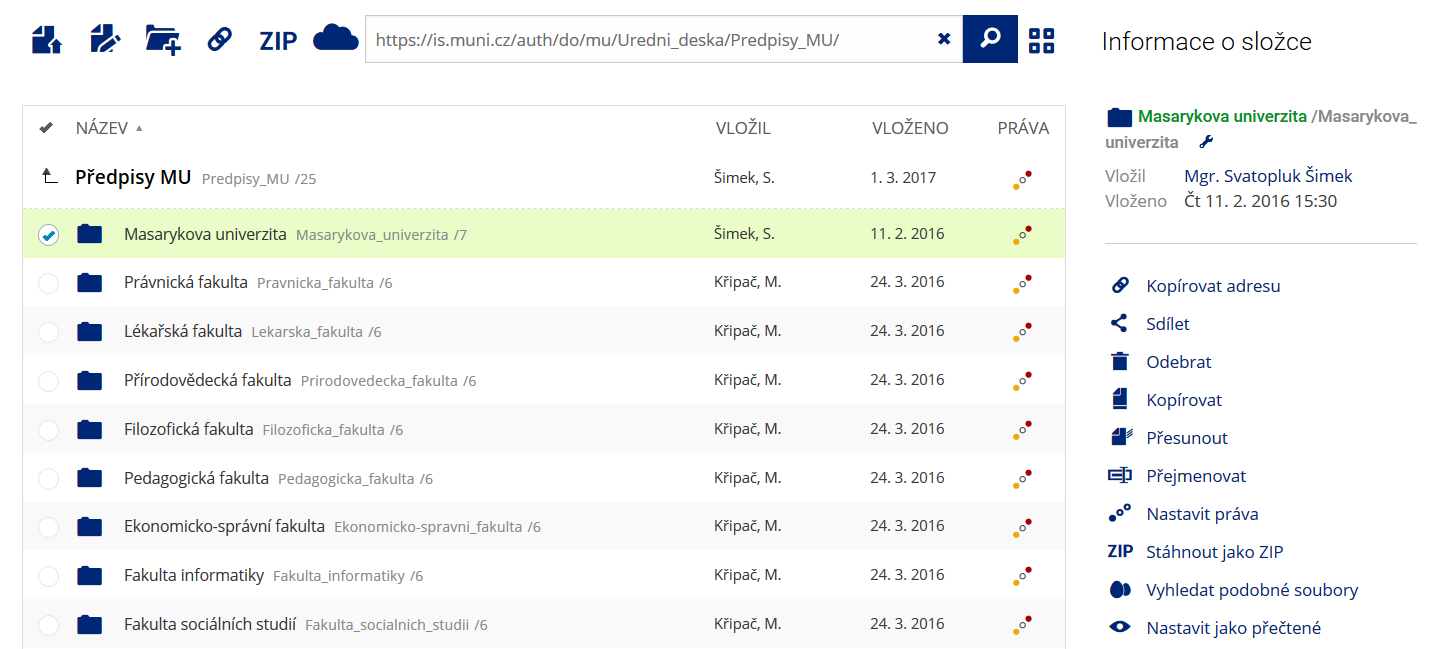 Pro častou práci je možné zvolit režim Více možností.
Pro častou práci je možné zvolit režim Více možností. Vyhledávaný výraz můžete zadat přímo do adresního řádku.
Vyhledávaný výraz můžete zadat přímo do adresního řádku.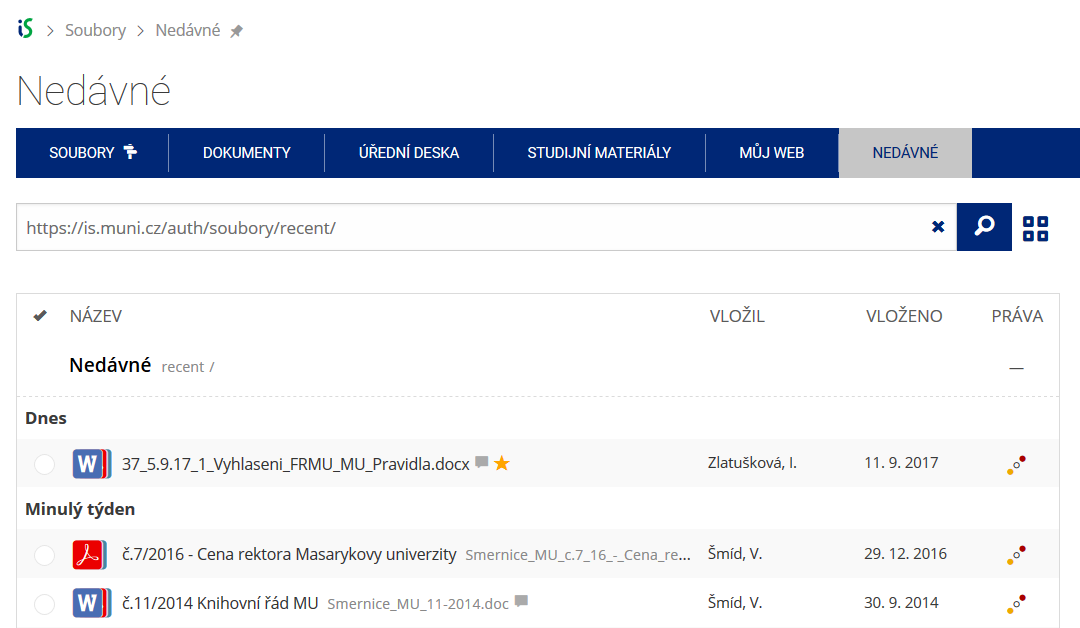 Pomocí funkce Nedávné je možné se rychle vrátit k právě prohlíženým souborům. Oblíbené soubory je také možné označit Hvězdičkou.
Pomocí funkce Nedávné je možné se rychle vrátit k právě prohlíženým souborům. Oblíbené soubory je také možné označit Hvězdičkou.